Researchers from the School of Biomedical Sciences at the LKS Faculty of Medicine, the University of Hong Kong (HKUMed), have made a significant advancement that could reshape the treatment landscape for hepatocellular carcinoma (HCC), the most common type of liver cancer, which often resists treatment and recurs. This cancer is especially prevalent in Southeast Asia and China. The research, published in the journal Science Translational Medicine [link to publication], revealed a previously unknown mechanism that allows HCC to grow more aggressively and evade existing therapies. The team also developed a new small molecule inhibitor that could improve treatment options for HCC patients.
A HKUMed research co-led by Professor Stephanie Ma Kwai-yee (first left) and Professor Clive Chung Yik-sham (first right), paves the way for significant advancement in hepatocellular carcinoma (HCC) treatment by identifying a key protein that fuels tumour growth and developing an inhibitor that can improve treatment outcomes.
Unravelling the mystery of tumour resistance
The liver plays a crucial role in various metabolic functions. In HCC, cancerous cells significantly alter these metabolic processes fuelling tumour growth. ‘In our study, we found that a specific metabolic pathway helps cancer cells maintain their stemness, which refer to their enhanced ability to grow, spread and survive,’ explained Professor Stephanie Ma Kwai-yee, co-lead author of the study, and Jimmy and Emily Tang Professor in Molecular Genetics in the School of Biomedical Sciences at HKUMed. Professor Ma is also Associate Vice-President (Research and Innovation) at HKU.
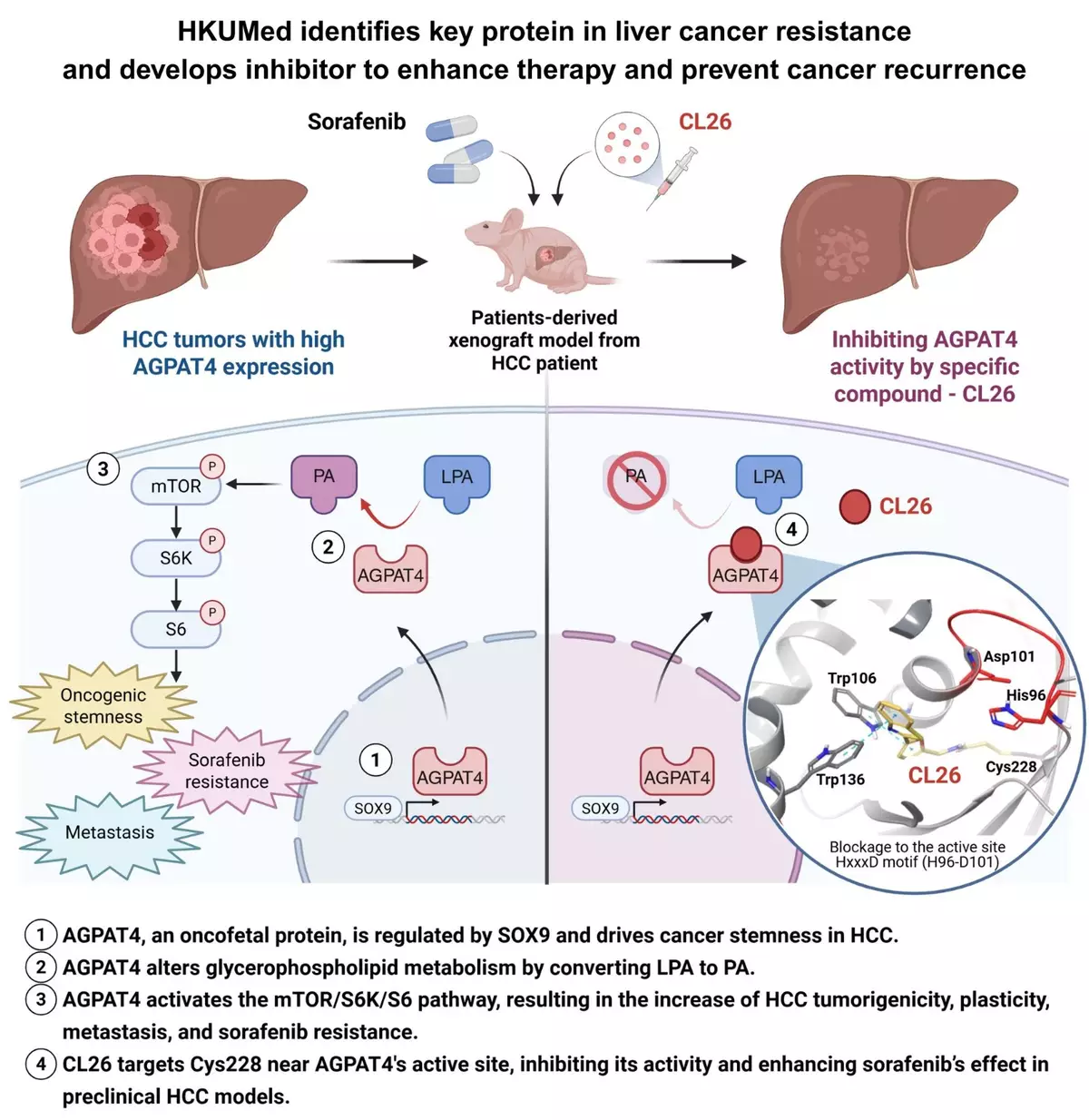
This pathway involves a protein called AGPAT4, which is abundant in both embryonic stem cells and HCC tumour cells, but is rarely found in normal tissues. ‘Our data show that AGPAT4 acts like a switch that makes cancer cells more flexible and aggressive,’ said Professor Ma. ‘This flexibility, known as tumour plasticity, is linked to a higher chance of the cancer to recur, spread and resist existing treatments like sorafenib, a widely used drug for liver cancer.’
The research team discovered that AGPAT4 increases the conversion of a fat molecule called LPA (lysophosphatidic acid) into another molecule called PA (phosphatidic acid). This process activates a signalling pathway involving cell manager mTOR and other proteins, which promote tumour growth and survival. Professor Ma added, ‘When we blocked AGPAT4 in a mouse model, tumour growth slowed down and the cancer became more sensitive to sorafenib.’
HKUMed researchers have identified key protein in liver cancer resistance and developed inhibitor to enhance therapy and prevent cancer recurrence. The research is co-led by Professor Stephanie Ma Kwai-yee (second right) and Professor Clive Chung Yik-sham (first right).
Developing an inhibitor to target AGPAT4
Building on these findings, the team developed a compound called CL26, which specifically targets AGPAT4. In preclinical models using patient-derived tumours, CL26 worked in combination with sorafenib to significantly suppress tumour growth. Toxicological assessments showed minimal side effects, suggesting the compound may be safe for future clinical use.
‘This is a promising step forward,’ said Professor Clive Chung Yik-sham, Assistant Professor in the School of Biomedical Sciences, HKUMed, who also co-led the study. ‘CL26 allows us to target liver cancer cells with precision, potentially improving outcomes for patients who no longer respond to standard treatments.’
Eyes on clinical trials to validate treatment potential
‘Our research suggests that AGPAT4 helps HCC cancer cells become more adaptable and resistant to therapy,’ said Professor Ma. ‘By targeting this protein, we may enhance the effectiveness of sorafenib and expand the therapeutic options for patients in clinical settings. We aim to offer hope to countless patients battling this challenging disease.’Professor Chung added, ‘CL26’s ability to precisely target AGPAT4 is likely one of the key reasons it works so well. We are conducting larger-scale preclinical studies to further assess the efficacy and safety of CL26 and hope to advance to investigational new drug studies and clinical trials.’
About the research team
The collaborative study was co-led by Professor Stephanie Ma Kwai-yee and Professor Clive Chung Yik-sham from the School of Biomedical Sciences at HKUMed. The co-first authors were Dr Johnson Ng Kai-yu and Amy Koo Tin-yan. Major collaborators included professors from The Hong Kong Polytechnic University, the Fourth Military Medical University in Xi’an, the Sun Yat-sen University Cancer Centre, and Guangzhou Medical University in Guangzhou; and Professor Guan Xinyuan from the Department of Clinical Oncology of the School of Clinical Medicine at HKUMed.
Acknowledgements
This research was funded by various grants from the Hong Kong Research Grants Council, including the Theme-Based Research Scheme, the Research Impact Fund, the Collaborative Research Fund, the General Research Fund, the Early Career Scheme and the Research Fellow Scheme. Additional support was provided by the Croucher Foundation’s Senior Research Fellowship and the Guangdong Science and Technology Department. The project also received separate grants through the Innovation and Technology Support Programme under the Innovation and Technology Fund, as well as funding for the Laboratory for Synthetic Chemistry and Chemical Biology, the Centre for Oncology and Immunology, and the Centre for Translational and Stem Cell Biology under the Health@InnoHK Programme initiated by the Innovation and Technology Commission of the HKSAR Government